Anterior Cervical Discectomy and Fusion for Radiculopathy
Why am I in pain?
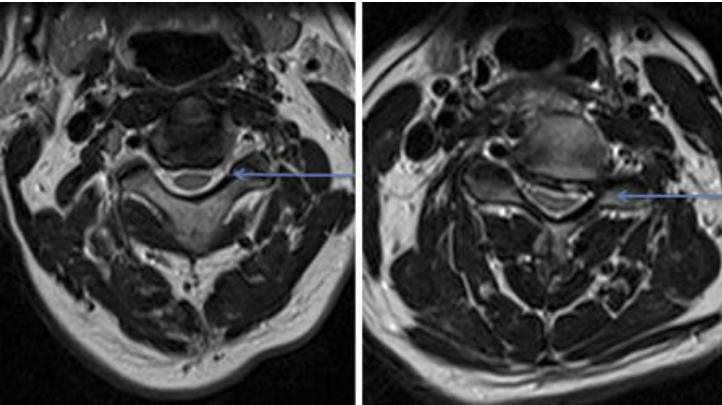
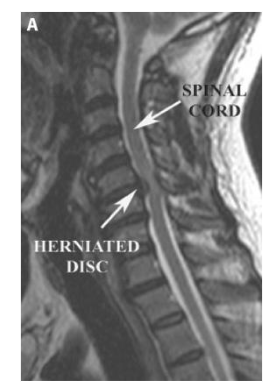
The most likely cause of your pain is compression of a spinal nerve by a combination of a prolapsed disc and overgrown bony spurs within the spinal canal, which together cause compression of the exiting nerve root.
Treatment Technique
You will drift off to sleep under general anaesthesia in a safe and controlled fashion by an anaesthetist. Whilst you are under anaesthesia you will not feel any pain, nor will you be aware of time passing. Having cleaned your neck in a sterile fashion, an incision about 1 inch long in the skin on the left front part of your neck will allow us to create a working channel between the oesopaghus (“gullet”) and the trachea (“wind-pipe”) on one side, and the great vessels (jugular vein and carotid artery) on the other side. The bones of the neck are then visualised, with the disc between the bones being removed. Further bony spurs may then be removed. We can confirm then that the spinal cord & exiting nerve root has been successfully decompressed. An interbody spacer (or cage) is then placed securely in the space where the disc used to be. Once a securing plate has been put in place over the two bones surrounding the newly implanted plastic cage, the wound will be stitched up, and the anaesthetist will allow you to wake up in a safe manner. The procedure itself will take approximately one and a half hours, but your stay in the operating room environs may be a little longer than this.