Treatments
Posterior Lumbar Interbody Fusion ("PLIF") ("lumbar fusion")
Why am I in pain?
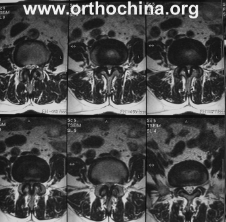
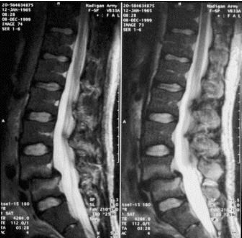
The most likely cause of your pain is compression of the spinal nerves by a combination of overgrown ligaments, prolapsed disc and overgrown bony spurs within the spinal canal, which together cause compression of the lumbar nerve roots. The spinal cord is not being pinched – it ends approximately 2 inches above where your problem lies. Movement of one bone over the other causes terrible back pain, and this movement also further narrows the spinal canal and the exit foraminae where the nerve roots exit. This movement is known as “spondylolisthesis”.
Treatment Technique
You will drift off to sleep under general anaesthesia in a safe and controlled fashion by an anaesthetist. While you are under anaesthesia, you will not feel any pain, nor will you be aware of time passing. Having cleaned your lower back in a sterile fashion, an incision about 4 inches long in your lower back will allow us to push the muscles off of the bones surrounding the spinal nerve roots. Screws will be put into the bones above and below the unstable level/levels, with strong connecting rods between the screws. The nerves will be exposed through the removal of portions of the 5 bones of your lower back.
The ligaments causing the nerve compression and any bony spurs will also be removed. The disc at the unstable level will be fully removed and will be replaced with an implant to help fusion between the two bones. Once the nerves have been successfully decompressed, the wound will be stitched up, and the anaesthetist will allow you to wake up in a safe manner. The procedure itself will take approximately three hours, but your stay in the operating room environs may be a little longer than this.
{kind=link}
{kind=link}
Everything you need to know
Get in touch
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Massa sit massa porta nibh tellus. Laoreet purus at duis faucibus eget sollicitudin id suspendisse.